Important new guidance on treatment of #MPXV (#monkeypox) in people living with #HIV: cdc.gov/mmwr/volumes/71/wr/mm7132e4.htm. Some key points summarised below.
🦠 we don't know if having HIV (by itself) makes you more likely to get MPXV, but we do know that people living with HIV are overrepresented among MPXV statistics in the current outbreak. Somewhere between 28% and 51% of MPXV cases are in people living with HIV (PLHIV).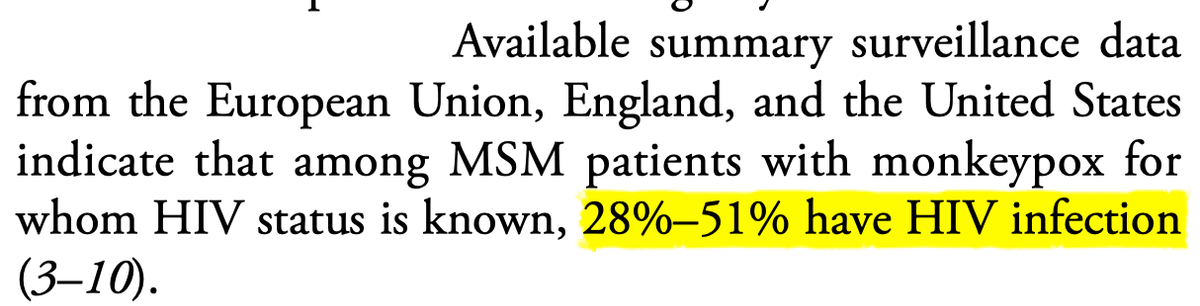
🦠 people living with HIV (PLHIV) do tend to have higher rates of sexually-transmissible infections (STIs), so the MPXV stats might reflect the fact that MPXV is an STI (don't @ me) or there might be other biological factors at play. It's too soon to tell.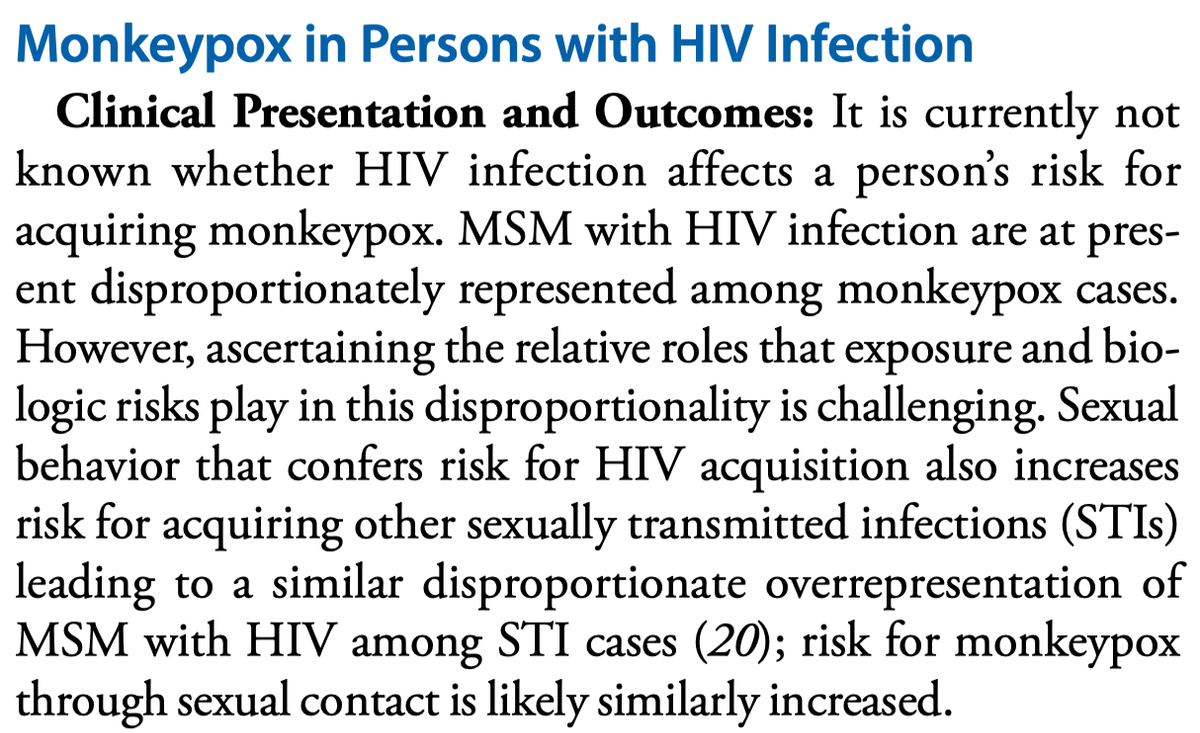
🦠 there are no known interactions between either the MPXV vaccine or the antiviral drug tecovirimat, so people taking HIV treatment, PrEP or PEP should continue to take that treatment as normal.
🦠 for PLHIV with advanced HIV illness/who are immunocompromised, the CDC thinks it's likely that they will have more serious complications from MPXV and/or potential fatalities, but the data is limited.
🦠 the CDC treatment recommendation is that PLHIV with MPXV should continue (or start) ARV treatment, and should be considered for tecovirimat if they have low CD4 counts or have more serious MPXV illness.
🦠 on vaccination, the CDC guidance states that the MVA-BN vaccine (Jynneos) has been shown to be both safe and effective in PLHIV with CD4+ counts over 200. For people with low CD4+ counts, effectiveness is unknown.
🦠 the older ACAM2000 vaccine is *not* recommended in people living with HIV.
🦠 importantly, while we have good data that shows that MVA-BN triggers a good immune response for MPXV in both HIV-positive and HIV-negative people, we still don't know for sure how well it protects against MPXV infection. No vaccine is 100% effective in real-world use.
🦠 for people diagnosed with MPXV, the CDC states that both HIV-positive and -negative people should follow the same isolation guidance, including isolating from pets who may be infected and become reservoirs.

Paul Kidd
@paulkidd
🏳️🌈 Activist, criminal lawyer, queer, HIV+. 🤔 law, disease, risk, gender, consent, Eurovision. ⚠️ My personal views, usual disclaimers. 📛 He/they/comrade.