Change My Mind:
I do not support waiting for a blinded randomized placebo-controlled monkeypox trial before expanding access to tecovirimat(TPOXX).
Despite being an online educator and supporter of evidence-based medicine. Is my thinking wrong? 💬
My main reason is that I think TPOXX can help stop the spread of MPX in this country. If it shortens the duration of illness, and illness duration is similar to contagiousness duration, that alone is worth it. See this Op-Ed @LeoNissolaMD @theIDPharmD
stateofthevirus.com/blog/fda-should-expand-access-of-tecovirimat-for-monkeypox-now
(And lest I be called out: it's also because TPOXX appears to be very safe and well-tolerated.) Main side effect in the TPOXX trial? Nausea, which is an extremely common side effect of many drugs, and usually easy to manage. Here's the list: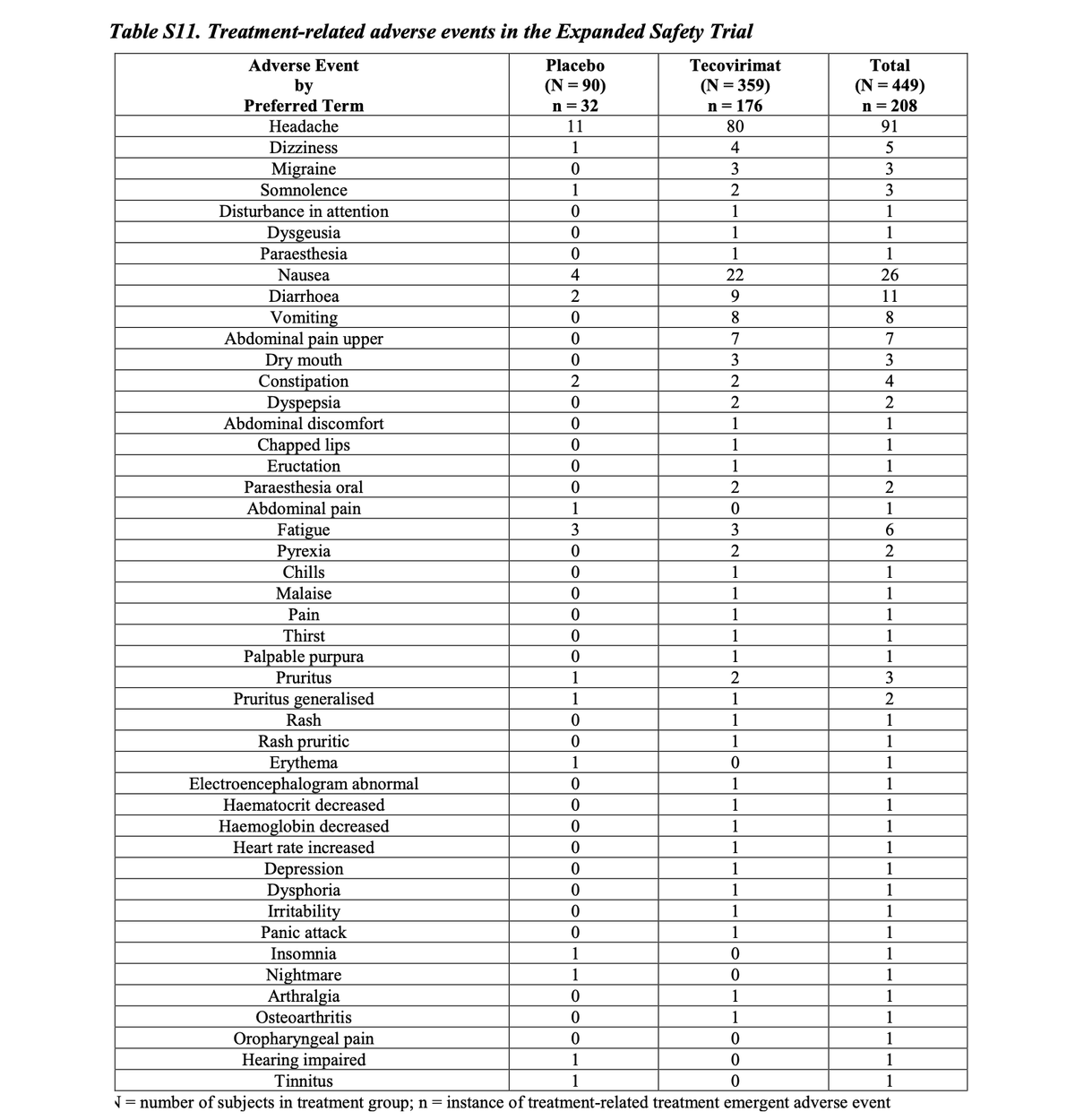
And of course we don't know about long-term risks or side effects, or effects in the larger population. But we don't know that of *any* drug after an randomized trial —which is why the FDA has Phase 4 of Drug Monitoring: once approved, drug side effects are still reported.
I should also add that the anecdotal data on TPOXX is also compelling. (Yes I'm aware that the plural of anecdote is not data).
Look at these recovery photos starting pre, day4, day7 TPOXX:
Yes, randomized controlled trials (RCT) are the best evidence that Drug A caused outcome X. And for COVID interventions—vaccines, paxlovid, steroids, etc—I demanded them. (I commonly speak out that Paxlovid has not been shown to help vaccinated people, for example.)
But we have other types of studies and evidence. They're not as strong of evidence, but: they exist because for one reason or another, conditions in our world don't make an RCT appropriate.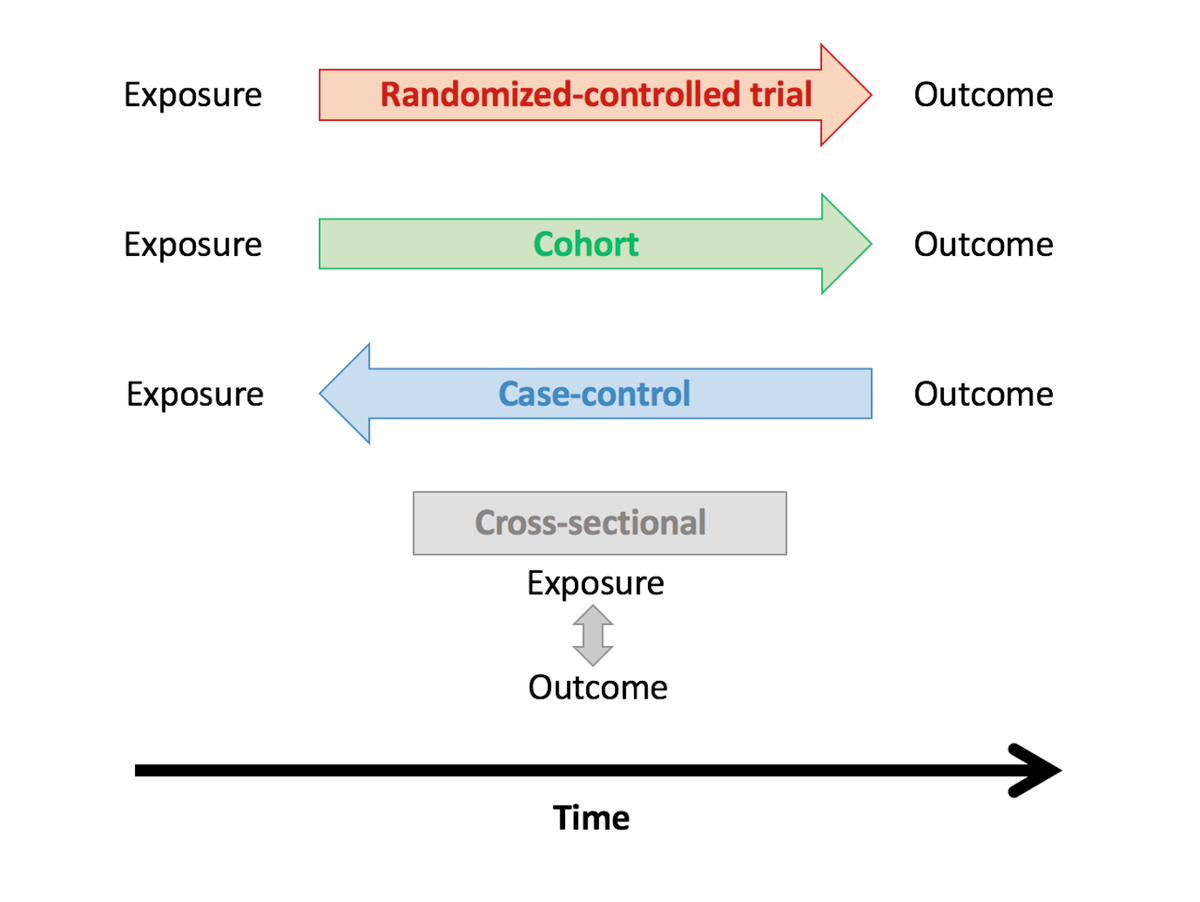
And for me, this is the clincher: we are in another pandemic. But THIS TIME, we ALREADY have something that could stop it from spreading more widely, say to children. Or to colleges. Or to jails.
Look at that 🇺🇸 line I highlighted: WE ARE RAPIDLY CATCHING UP IN PER-CAPITA CASES.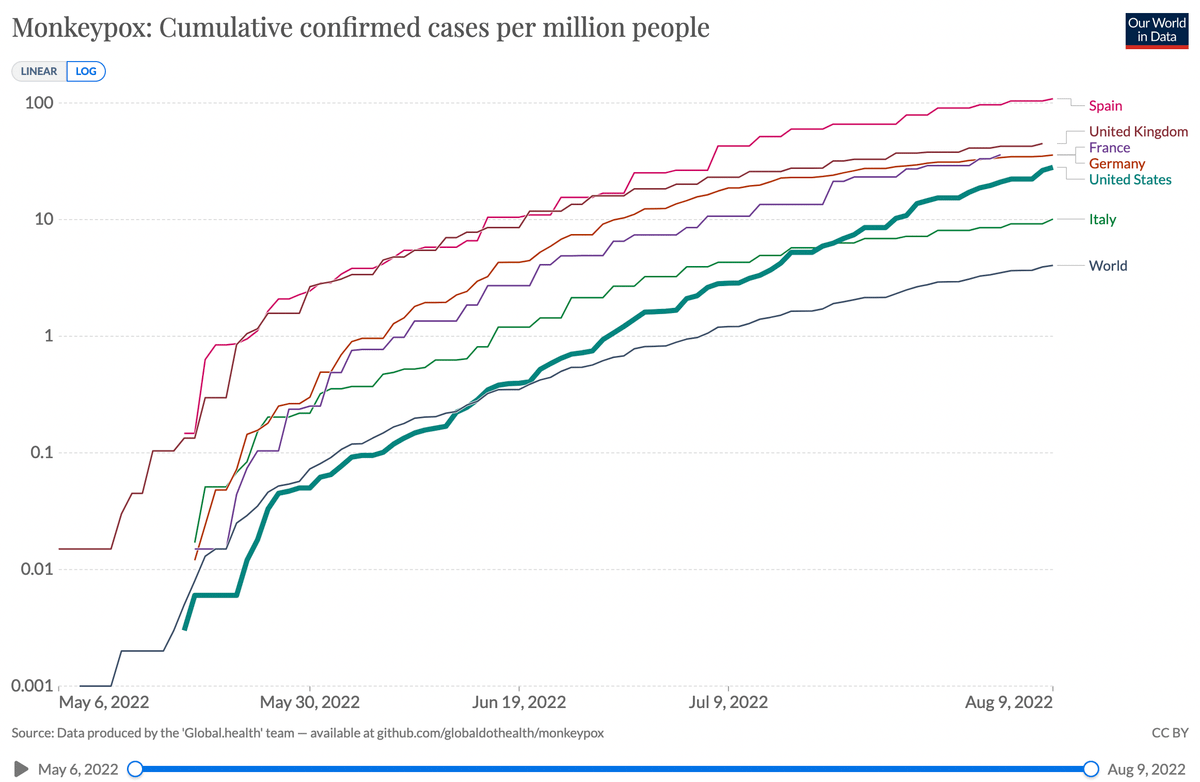
Finally, I'll admit my bias: this is personal and emotional. I'm a gay ER doctor in SF.
—This is pandemic #2
—I've treated MPX patients my same age
—I have seen genital lesions so upsetting and intrusive that I have had counseling on how to erase them from my mind.
So please, tell me if my thinking is wrong. Sure, ideally we'd do an RCT. But is it really worth waiting 6-9 months for a trial to get published when TODAY we have less than 10,000 monkeypox cases in this country? Because 11 days ago, we only had 5,000.
I'll let you do the math.
And you know what? We already have PLENTY of placebo controls for any trial that needs them. They're called "gay men with monkeypox who we wouldn't treat."
We need expanded TPOXX access now. We need an emergency use authorization.
Adding a bunch of evidence-based medicine experts who I respect @TheSGEM @tamingthesru @Runde_MC @First10EM @EMNerd_ @PulmCrit @nickmmark @EMSwami @emlitofnote @GidMK @srrezaie @spoonfedEM @thenntgroup @SZehtabchi
I also want to highlight this article from the LA Times that helped me cement my thinking in this (I literally just wrote this thread this morning, had no idea the article would come out today.)
twitter.com/AlpertReyes/status/1557371309985738752?s=20&t=HYu2_-00YUmFh5pxmPgyBg
And a big TY to the patients on Reddit's monkeypoxpositive forum for sharing their stories and photos reddit.com/r/monkeypoxpositive/comments/wb9fjf/my_tpoxx_journey_great_progress_just_finished_day/

Graham Walker, MD
@grahamwalker
Emergency physician; I made @mdcalc; Tweets = my own/not employers'. Not a hero, just a well-trained human. So, so tired of COVID. #GetVaccinated 💉