



















Thanks to @mrichtel for highlighting the teen/adolescent mental health crises filling our emergency departments across the US, from the perspective of what they experience. Some commentary from an ER doctor who sees this play out every single shift: 🧵
nytimes.com/2022/05/08/health/emergency-rooms-teen-mental-health.html
1️⃣Mental health crises requiring psychiatric holds (usually for suicidal thoughts/sometimes for homicidal thoughts or inability to care for oneself due to mental illness) are worse for patients under 18 because of fewer beds, but the delays exist for ALL psych patients.
Let's look at my state, California. We've LOST adolescent inpatient psychiatric beds. And only 11 of California's 58 counties even HAVE a single inpatient adolescent psych bed. If your child is suicidal, their only option may be a facility 5+ hours away.
Don't even get me started on children — the 12 and under crowd (yes, these patients can experience mental crisis as well).
And here's a look at the drastic cuts in psych beds for adults in CA — it's not any better: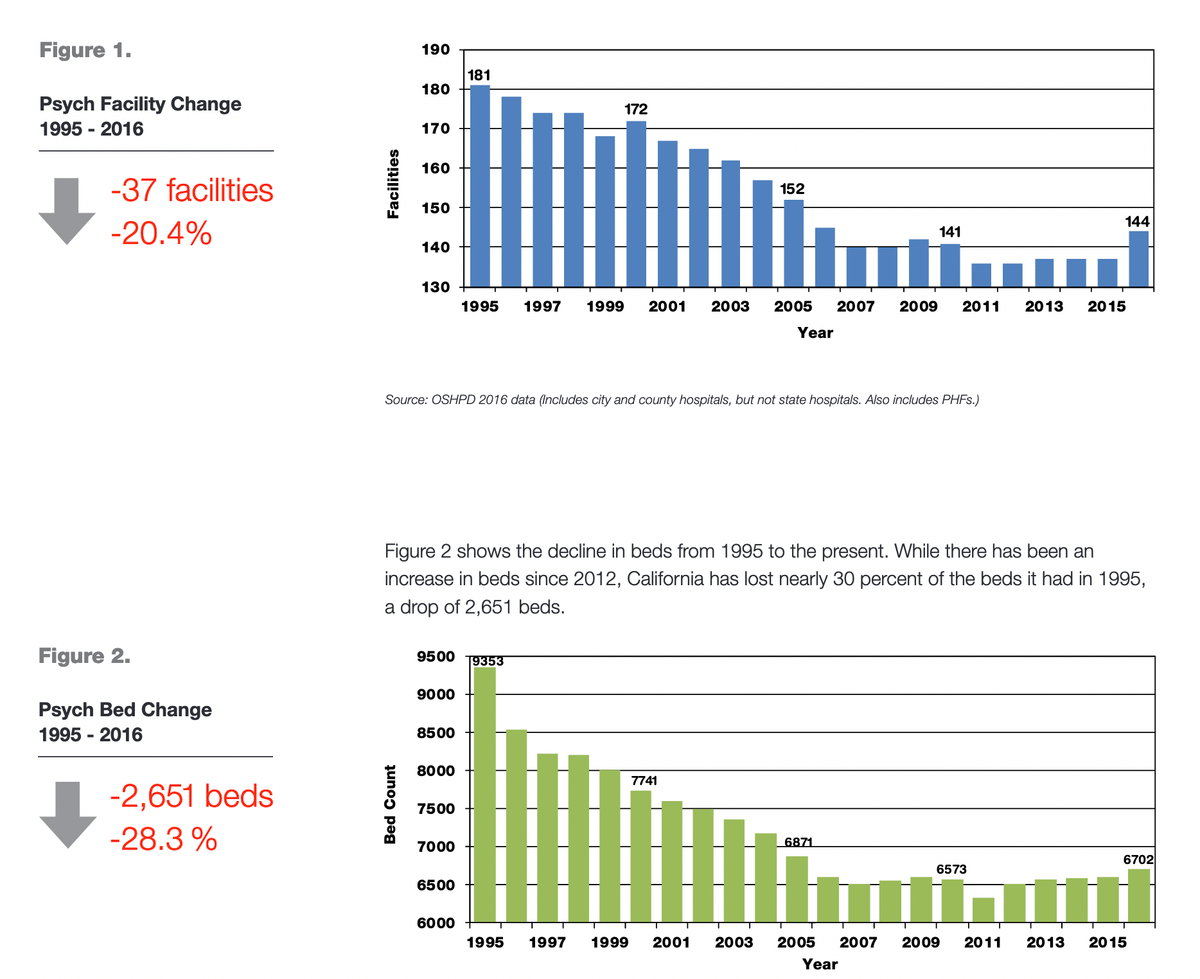
2️⃣All states have some sort of mental health crisis law that recognizes *someone* to legally hold a patient against their will for a period of time — sometimes it's the police, a judge, a psychiatrist, or an ER doctor. In California, it's a "5150" (named after the CA code)
What's *supposed* to happen is that these patients *briefly* visit the ER & are screened for any medical issue they might have (either that supersede a mental health problem, like an overdose) or for medical problems that mimic mental health crises (like a brain tumor).
After this brief ER visit, these patients are transferred to an inpatient psychiatric facility, where often medications + therapy are started to help address their symptoms, and they undergo additional psychiatric evaluations to determine if or when they're safe to go home.
Unfortunately the "supposed to happen" version happens less than 5% of the time for adults, and less than 1% of the time for adolescents, mostly due to delays in availability of psychiatric beds, as expertly described by the article above.
(The other big cause for delays is waiting for alcohol/drugs to clear, which can affect a person's thoughts/mood/behavior. It's usually alcohol—a depressant—or methamphetamine, which can cause depression coming off it, as well as permanent psychosis mimicking schizophrenia.)
These patients easily often wait 1 or more days. IN AN EMERGENCY ROOM. Waiting for one of these beds to be available. (As you can imagine, an ER is often not a quiet, calm environment to encourage and stabilize one's mental health.)
3️⃣We have a law called EMTALA; anyone in an ER must be seen/evaluated and stabilized. And if the patient needs services you don't have at your hospital (like brain surgery), it says that any hospital that DOES have those services AND has an empty bed MUST accept the patient.
But EMTALA seemingly does not apply to psychiatric hospitals (or this is not enforced). Psychiatric hospitals pick and choose which patients they want:
* How severe is their mental illness?
* Do they have insurance?
* How long might they need to stay?
* etc
cc @NickSawyerMD
Psychiatrists (NB: my dad is a psychiatrist, I'm the most pro-mental health ER doctor out there) can even refuse to accept patients until blood work is done on them, even when the treating doctor (me) thinks it is entirely unnecessary.
I have even had psychiatrists force me to *repeat* unnecessary blood work because they did not know how to interpret the blood work properly. Should I have stood my ground, refusing to do unnecessary tests, if the alternative is further delays for definitive care for my patient?
God forbid you have any serious medical problems (which, no surprise, often run in tandem with serious mental health problems). You sleep with CPAP? You broke your arm and have a sling? You have a feeding tube? Well those are all strangulation hazards; you'll wait 4x as long.
You want to talk about mental health parity or inequality? If you're uninsured (or in some places in the US, insured with Medicaid), you will absolutely wait longer for a psychiatric stabilization bed. And depending on the county/state, you cannot transferred across county lines.
4️⃣This issue is nothing new — but worse with the pandemic (see this additional piece by Richtel showing just how bad it's gotten).
We are *all* suffering with our own mental health post-pandemic, but going through this as a teen has just been devastating
nytimes.com/2022/04/23/health/mental-health-crisis-teens.html
I wrote about this in 2014 and it has only gotten worse. Today patients' mental health has fully unraveled by the time they show up in the ER, and since the ER has to be everything for everybody, it is not perfect for anybody.
journals.lww.com/em-news/Fulltext/2014/08000/Emergentology__BabysittERs.6.aspx journals.lww.com/em-news/Fulltext/2014/08000/Emergentology__BabysittERs.6.aspx
5️⃣(I'll also note that it's not like your ER receives any resources specifically to address any of the issues that Congress/state lawmakers or advocacy groups criticize us for). A list of subjects that we're expected to address:
Mental health
Any and all medical complaints
Trauma
End of life care
Opiate epidemic treatment
COVID management
COVID testing
COVID vaccination
Alcohol and drug use and withdrawal
Dementia care and elderly care
Social issues like homelessness
Domestic violence
Nursing home care evaluations
Chronic pain management
Human trafficking
Sexual assault
Public intoxication
Post-surgery evaluations
Hospital employee injuries/needlesticks
"Medical clearance" for people under arrest by police
Child abuse, elder abuse/neglect
Strict time-based metrics for medical problems like heart attacks, strokes, sepsis/infections
6️⃣Sorry, off the soapbox.
Next is the Catch-22 that happens when someone is *still* in your ER when their legally-allowed 72 hour hold expires. I can't legally hold someone longer than 72 hours, but I also can't legally discharge someone who is still actively suicidal.
Now this actually played out in Washington state in 2014; they made it illegal to hold patients in the ER for longer periods of time. (Someone from WA please comment how this played out!)
governing.com/news/headlines/washington-state-supreme-court-rules-leaving-mentally-ill-in-emergency-rooms-is-illegal.html
That being said, I'm now seeing that Washington State just extended the legal hold time to 5 days (*excluding weekends and holidays*!) so I'm wondering if that ruling from 2014 hasn't gone so well. wsha.org/articles/bulletin-changes-to-the-involuntary-treatment-act-ita-part-1-key-changes/
7️⃣Unlike a migraine or stomach bug, there are not medicines that we can give to rapidly make someone "not depressed." But there have been numerous studies of a drug that may make people "not suicidal." And that drug is Ketamine.
I will caution that since we started out talking about adolescents, ketamine is of course not nearly as well studied for depression/suicidal thoughts in teens. *However*, it actually is our drug of choice for sedation for patients under 18, and we use it frequently in the ER.
If you've ever seen David After Dentist ("Is this real life?") — yeah, that's ketamine. Ketamine dissociates our brains from our bodies, but unlike other sedatives doesn't make you stop breathing, making it great for putting people to sleep in the ER.
I won't get into too much science-y detail but the BMJ has a nice paper on ketamine for acutely suicidal patients; at least in the short term it may help a lot, especially in patients with bipolar disorder.
bmj.com/content/376/bmj-2021-067194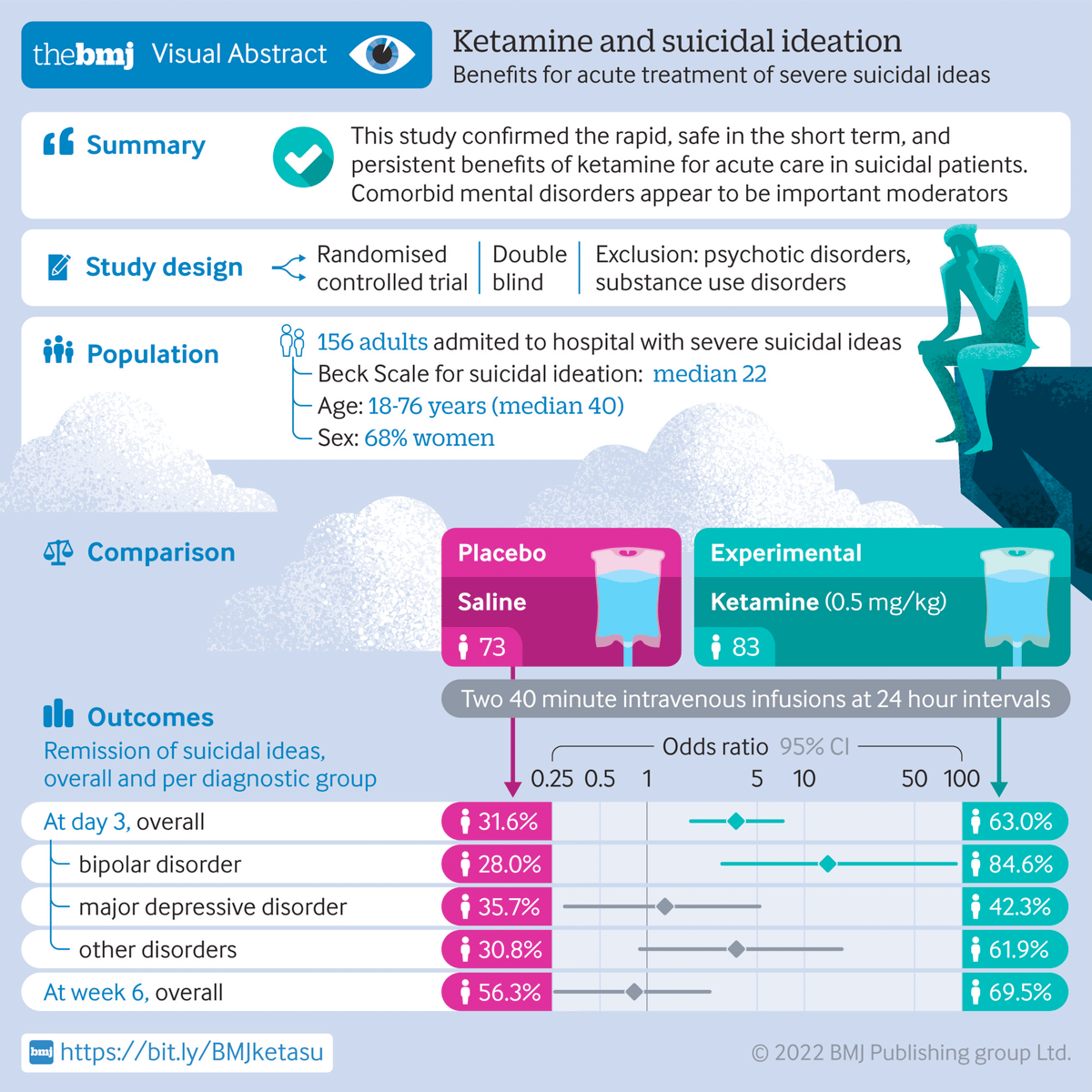
The American Journal of Psychiatry also found that it was very effective — again, more in the short term — but with just one dose. ajp.psychiatryonline.org/doi/full/10.1176/appi.ajp.2017.17040472?casa_token=eOKeS193sCwAAAAA%3Ap3IPEE3cA67uWTE4sZEbCR2pO1vB7O-jFb5P_0bnEmp8xYAaxFwdu3cVLO4CFYX__mTRhKzK0SMp ajp.psychiatryonline.org/doi/full/10.1176/appi.ajp.2017.17040472?casa_token=eOKeS193sCwAAAAA%3Ap3IPEE3cA67uWTE4sZEbCR2pO1vB7O-jFb5P_0bnEmp8xYAaxFwdu3cVLO4CFYX__mTRhKzK0SMp
There are also a few review articles — this one in pediatric patients — showing that it may help some patients, but we still don't know the long-term effects of ketamine on children. (That being said, we've been using ketamine for decades for sedation.)
pubmed.ncbi.nlm.nih.gov/32385697/
It also seems like ketamine has been used successfully not just in the outpatient world — but also the ER for acutely suicidal patients. ncbi.nlm.nih.gov/pmc/articles/PMC4614623/
sciencedirect.com/science/article/abs/pii/S0735675721000073
Is anyone's ER doing this? Does anyone have opinions if we should be? I will say that ER doctors are often the ones pushing the envelope of what's possible and how to help patients — often because we are the ones that see all the failings our "system" every. single. day.
And given the alternative so eloquently described by @mrichtel—spending not hours but DAYS or WEEKS in a lifeless, sterile, cold ER hallway or room awaiting a scarce psychiatric crisis bed that can choose to not accept you if you're uninsured... maybe it's worth it.
🔚In conclusion:
Yes, it's really as bad as Richtel describes.
We need more psych beds.
We will not get more psych beds without better funding for them.
We are doing our best in the ER with what we're given, and it's not enough and not right.
We probably need to rethink mental health treatment in the US, especially in our COVID world.
And in memory of all we have lost to suicide, including several people close to me: call the Suicide Hotline: 800-273-8255 or text Text HOME to 741741 to reach a Crisis Counselor.
And specifically for physicians: Physician Support Line, 888-409-0141.
FIN