Here are some of my favorite hyperkalemia pearls that will help take your understanding of the disease process to the "201" level!
And, yes, this ominous banana is meant to be an abstract visualization of the serious consequences of hyperkalemia.
Read on!
- Thread -
Only 2% of total body K is extracellular.
In HyperK, the resting membrane potential becomes LESS negative, leading to downstream effects on electrical conductivity.
Chronic changes in extracellular K lead to compensatory mechanisms to reduce this excitability.
twitter.com/ROKeefeMD/status/1743256123019526364?s=20
Under normal conditions, 90% of potassium is eliminated renally, and 10% is eliminated in stool.
The most common cause of HyperK presenting to the hospital is decreased renal function or missed dialysis.
Diet is usually only a factor in those with reduced renal function.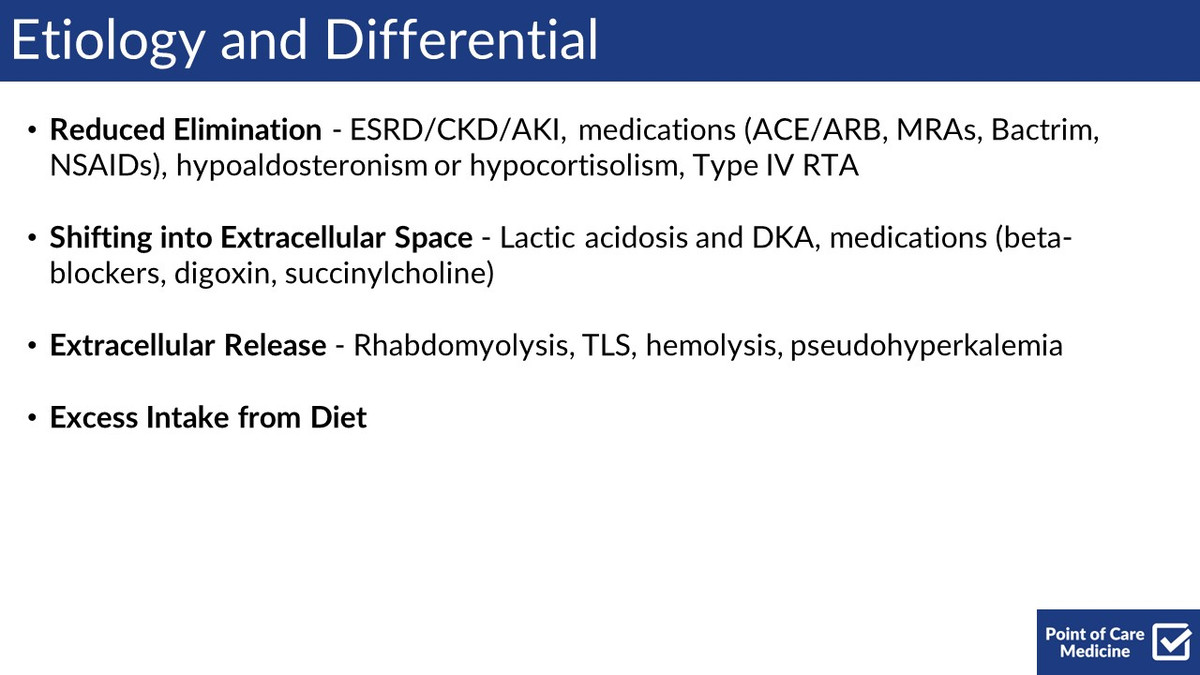
Healthy kidneys can excrete up to 400 mEq of potassium each day.
The average potassium intake of ~2,000 to 3,500 milligrams (mg) per day translates to approximately 51 to 90 mEq (mmol) per day.
ods.od.nih.gov/factsheets/Potassium-HealthProfessional/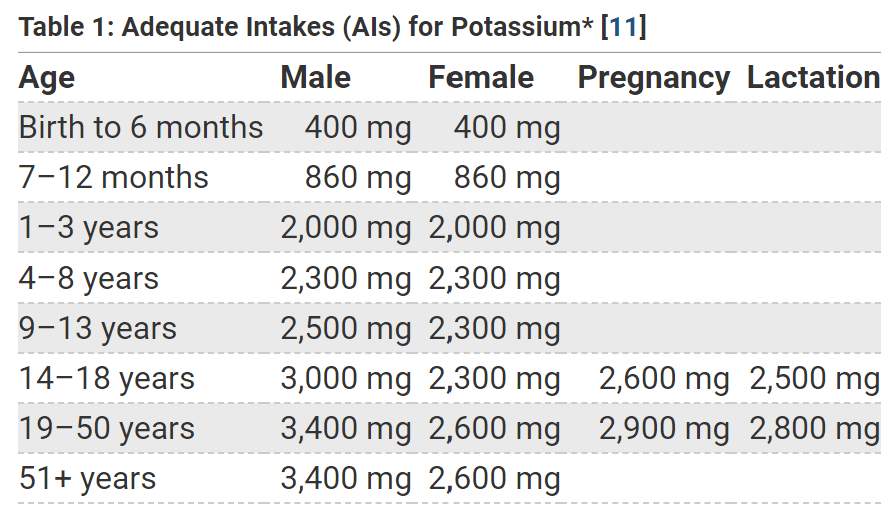
Common foods high in potassium
- Potatoes
- Dairy
- Cereals and Bran
- Bananas
- Avocados
- Leafy green veggies
kidney.org/sites/default/files/NKF_Guide_to_Low_Potassium_Diet_Final_0.pdf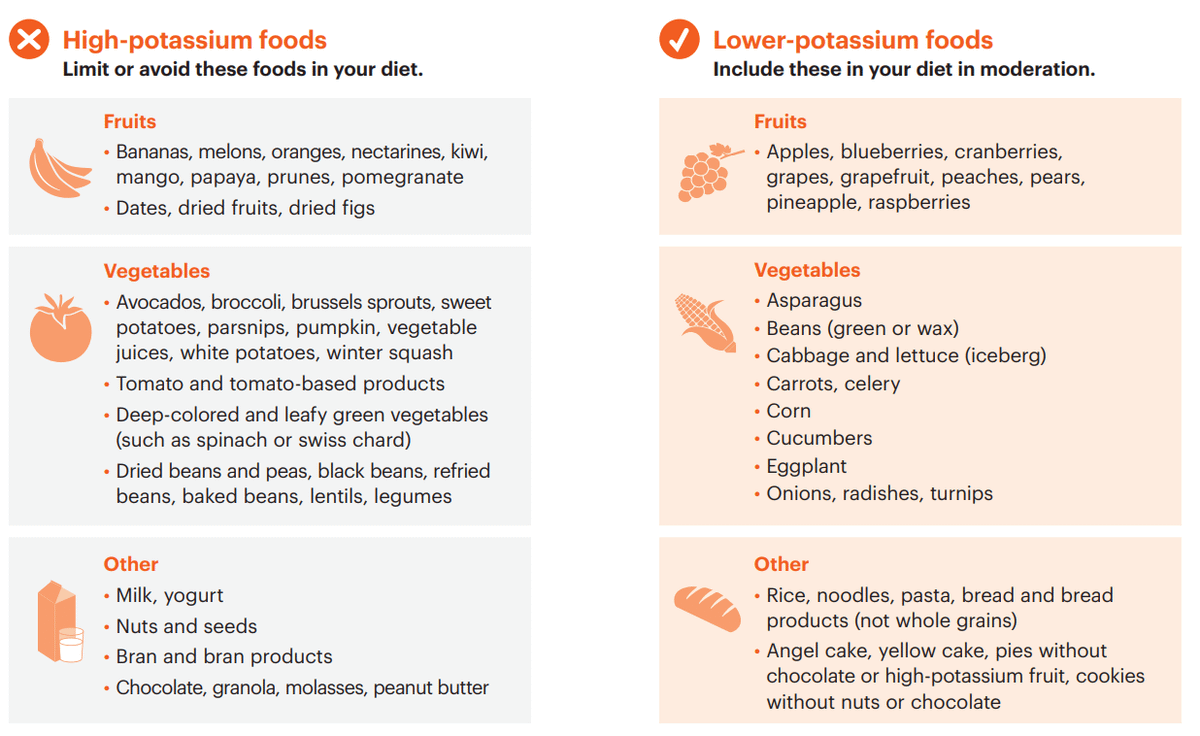
If you really want to get into the weeds, bananas contain 1.5-2.0 mEq of potassium per inch.
Thus, the average banana has ~12 mEq.
Shout out @nickmmark for those pearls!
x.com/nickmmark/status/1714630670121935004?s=20
ACE/ARBs, MRAs, NSAIDs, and TMP-SMX can all lead to HyperK by lowering the release/effect of aldosterone.
Through the complex process of RAAS, aldosterone leads to sodium retention and potassium excretion, mostly at the distal convoluted tubules.
Acidosis causes HyperK by messing with the Na/H antiporter and the sodium gradient, which in turn reduces the activity of the Na/K-ATPase pump.
Insulin, on the other hand, stimulates the Na/K-ATPase pump, leading to more K going into the cell.
If a patient is in DKA, they may be hyperkalemic since insulin is not present to push potassium into cells.
But TOTAL body K will be low.
So you need to replete K when less than ~5.2 mEq/L and hold insulin if less than ~3.3 mEq/L to prevent a dangerous hypokalemia.
VBG/ABG K levels may not perfectly correlate with the BMP but should be within ~0.5 mEq/L.
Hemolysis in vitro as part of the blood drawing process can lead to "pseudohyperkalemia".
Most labs will report this as “hemolyzed” rather than as an inaccurately high level.
Severe or acutely elevated K is more likely to be symptomatic; those with chronic elevations will often be asymptomatic and diagnosed incidentally.
The weakness associated with hyperkalemia often starts in the legs and then progresses to the arms (ascending paralysis).
Calcium gluconate should reverse EKG changes in 5 minutes; if not, push again.
Calcium chloride has a higher risk of tissue necrosis at the IV site and should be given centrally.
Calcium salts have no actual effect on K levels, and don’t last more than 30-60 mins.
Temporizing/redistributing can drive the K down ~0.5-1.5 mEq/L in the short term.
Inhaled SABA (albuterol) should not be used as a monotherapy and is less likely to work in patients taking beta blockers or with CKD.
Elimination via furosemide or Lokelma requires urine or stool output.
If the patient cannot do either, the only other way to eliminate potassium is via dialysis.
However, elimination is not required in all patients - especially if the acute insult has been addressed.
Cation-exchange resins like kayexalate and lokelma work by releasing sodium ions which are in turn exchanged with potassium in the gut.
Resins commonly lead to constipation and should be given with laxatives.
Sodium polystyrene sulfonate (Kayexalate) has been shown to have rare but serious adverse effects, specifically gut necrosis.
pubmed.ncbi.nlm.nih.gov/31180477/

Ryan O'Keefe
@ROKeefeMD
MD/MBA @PennMedicine @Wharton | Hospitalist | Creator @pointofcaremed | Follow for clinical threads and pearls