Quick thread on changes to emergency medicine billing requirements coming in a few months (Jan 1, 2023)!
Most importantly: goodbye to the absolutely inane HPI, ROS, and PE elements for billing. Hooray! Instead, EVERYTHING is based on medical decision-making (MDM). ⬇️⬇️
Props to my friend and colleague @RobPNorris who spent a ton of time summarizing all of this. I'm stealing his slides. This is all based on AMA guidelines here ama-assn.org/system/files/2023-e-m-descriptors-guidelines.pdf
Unfortunately MDM is a Russian doll of onion layers of complexity that only CPT and the AMA could have mustered. But the top level elements are:
1️⃣Number/complexity of problems addressed
2️⃣Number/complexity of data assessed
3️⃣Risk of complications/morbidity
Essentially you're gonna get "points" or "levels" for those 3 elements, and your two HIGHEST levels will determine your overall MDM complexity which will then be a billing code
99282 = Straightforward
99283 = Low
99284 = Moderate
99285 = High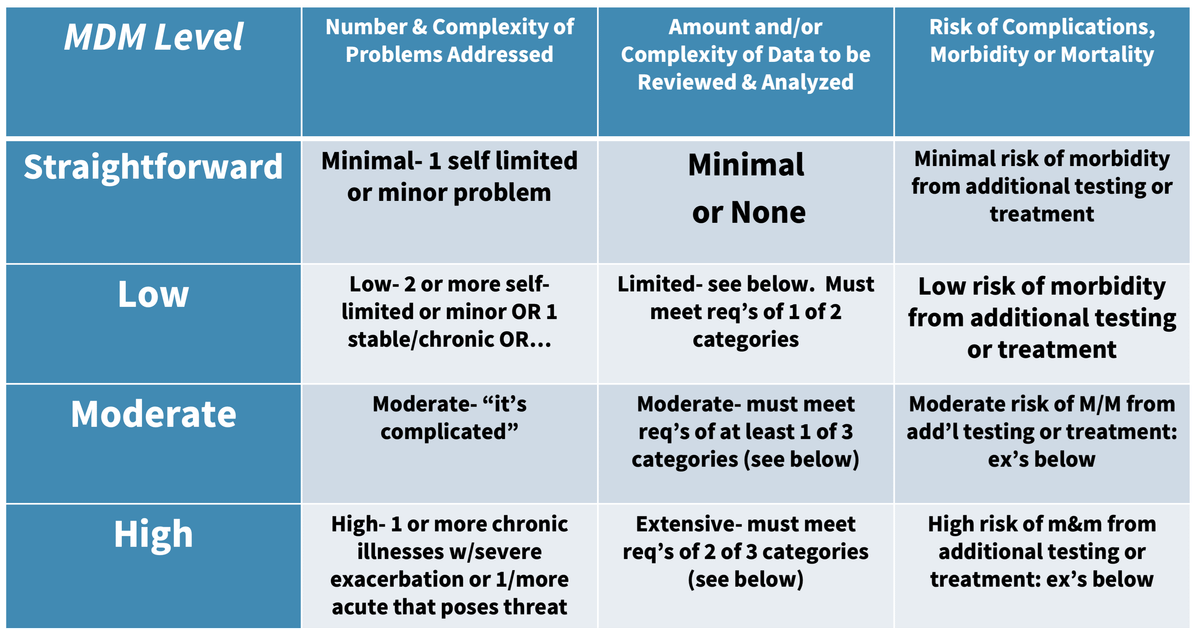
I know. It's obnoxious. Each Problems/Data/Risk section gets assigned its own "straightforward/low/moderate/high" and has its own definitions for these scores. It's annoying.
But still, it ain't 10 review of systems.
I'll go through and just list these out, and then give what I... think? ... would be examples? @RobPNorris took these directly from the AMA PDF.
Number of problems/complexity of problems: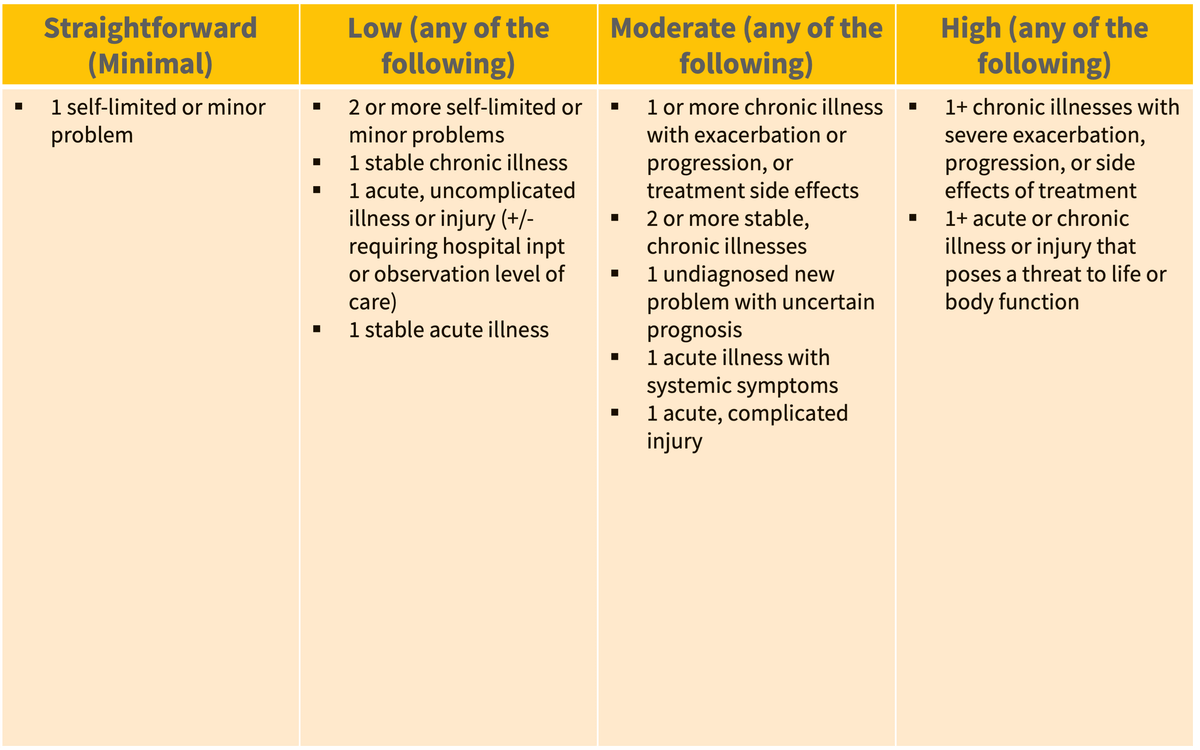
Amount of Data/Complexity of Data
This is where the Russian Doll starts to get pretty ugly; you'll notice "Must meet X of 3 categories" to determine "Level of Data Complexity" (this one could benefit from simplification)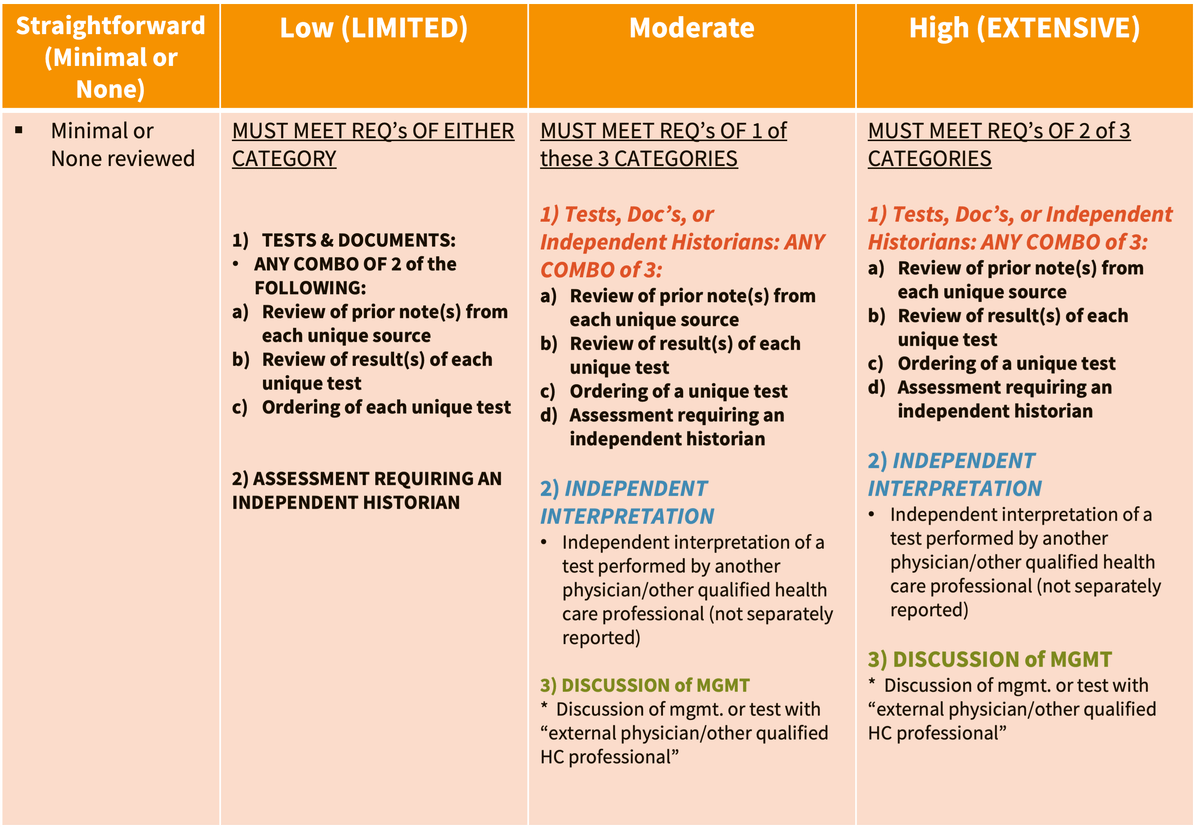
Level of Risk/Morbidity I think is relatively straightforward; they give examples but I think emergency physicians should be able to categorize this risk very easily.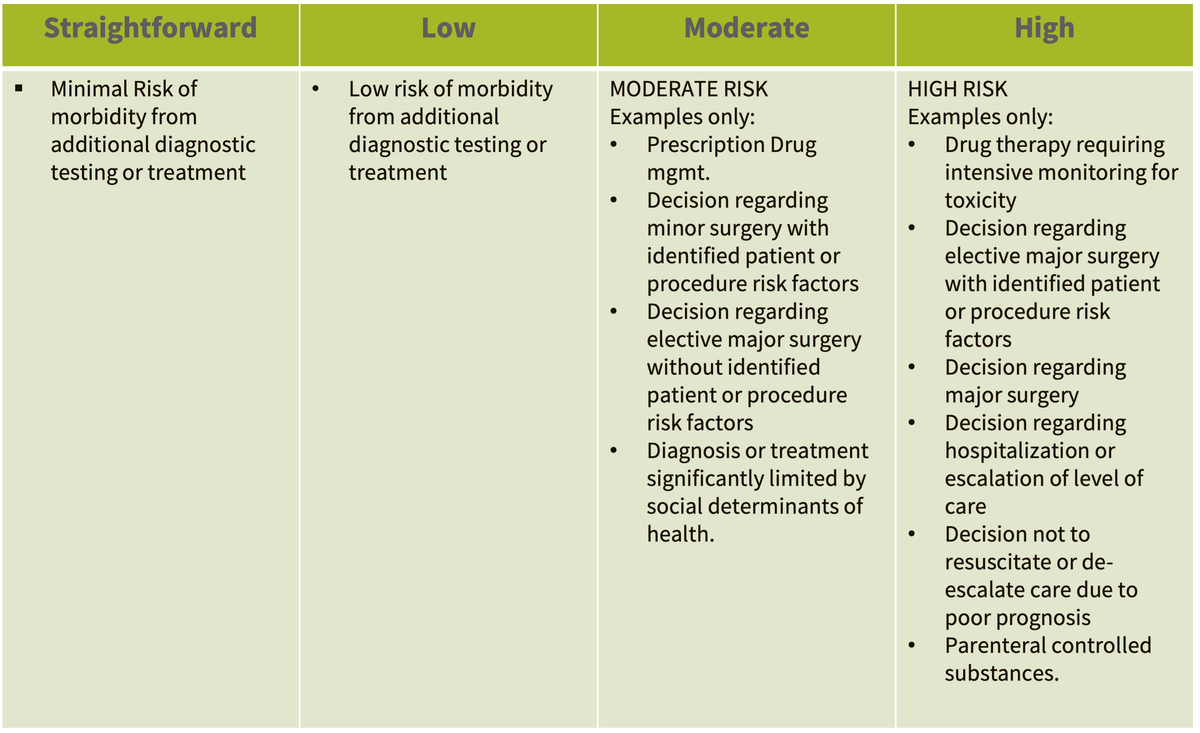
Important points:
Shared decision making is specifically included! If you would normally/often do X for a patient but the patient opts out, X still counts toward testing/risk/complexity. (X could be "admit to the hospital" or "get a CT scan" or "order a troponin.")
LOS 1/99281 is pretty much no longer a thing for emergency medicine. I don't even really understand what an ER visit that "does not require a physician or other healthcare professional" means.x
Critical Care is still a separate billing code; procedures as well are separate.
So what do I think this will look like for the future of EM documentation?
—Focused HPI like you're probably already doing
—*Relevant* ROS, Social, Family History, PMH in the HPI
—Focused, *relevant* physical exam documentation
—(A little) more time on MDM, probably not much
As @gerardo_gb says — I'd really love EM to lead all of medicine in moving to APSO (Assessment/Plan at the 🔝 of the note, Subjective/Objective below it). It is MUCH easier for people reading your note to skim and see the important, relevant parts with APSO.
twitter.com/gerardo_gb/status/1573413901924024337?s=20&t=oTm5Q0fRAG40D0ezzE75HQ
What might this look like in practice? I mean could this "rule out appy" note be a pipe dream? Could my ER note 👇really be this straightforward, containing almost exclusively-relevant information to the patient's CC? And fit in 20 lines?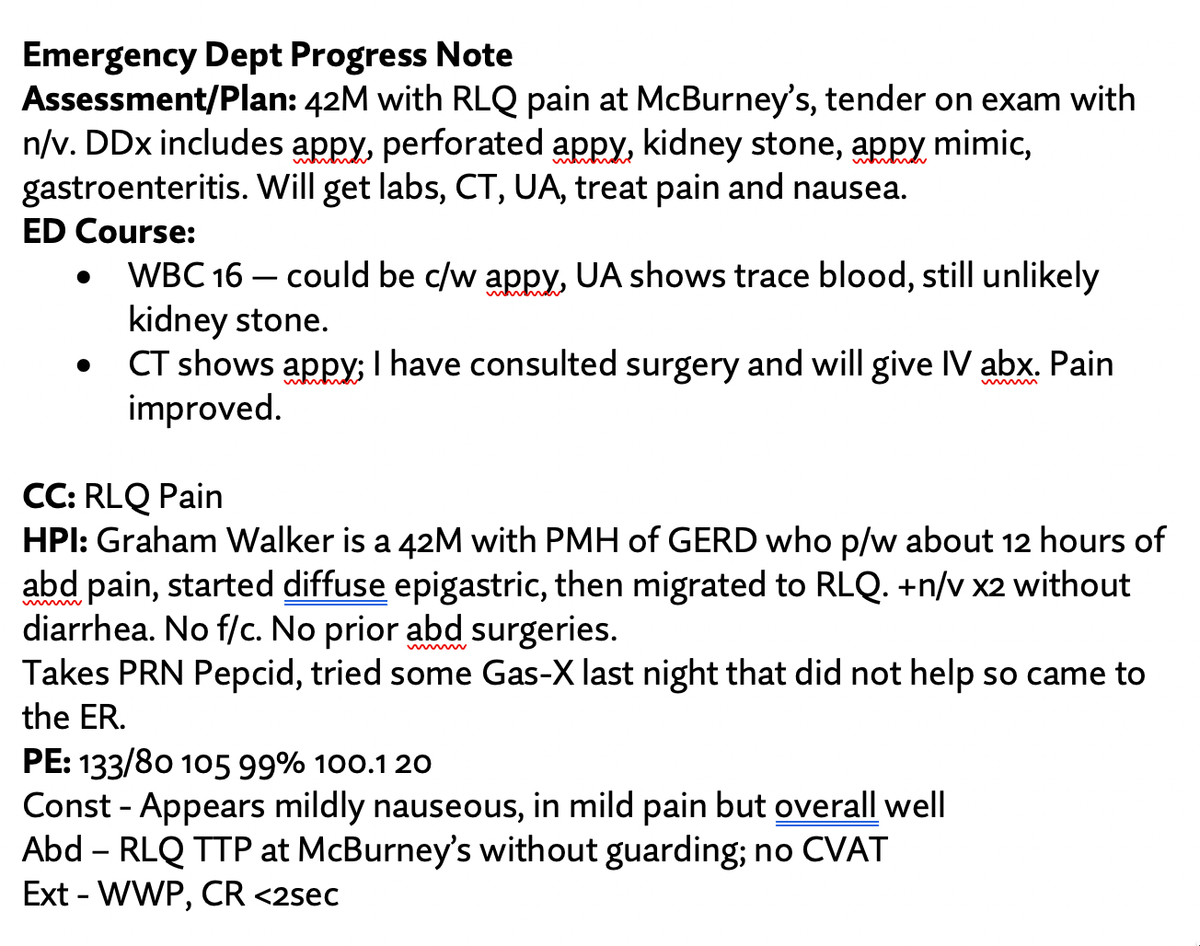
Of course it's not gonna always be this straightforward. But for the straightforward cases, could I really document this little and still demonstrate the medical complexity, risk, and problems along with any med-legal stuff? I think this would be a 99285 chart. Let's look: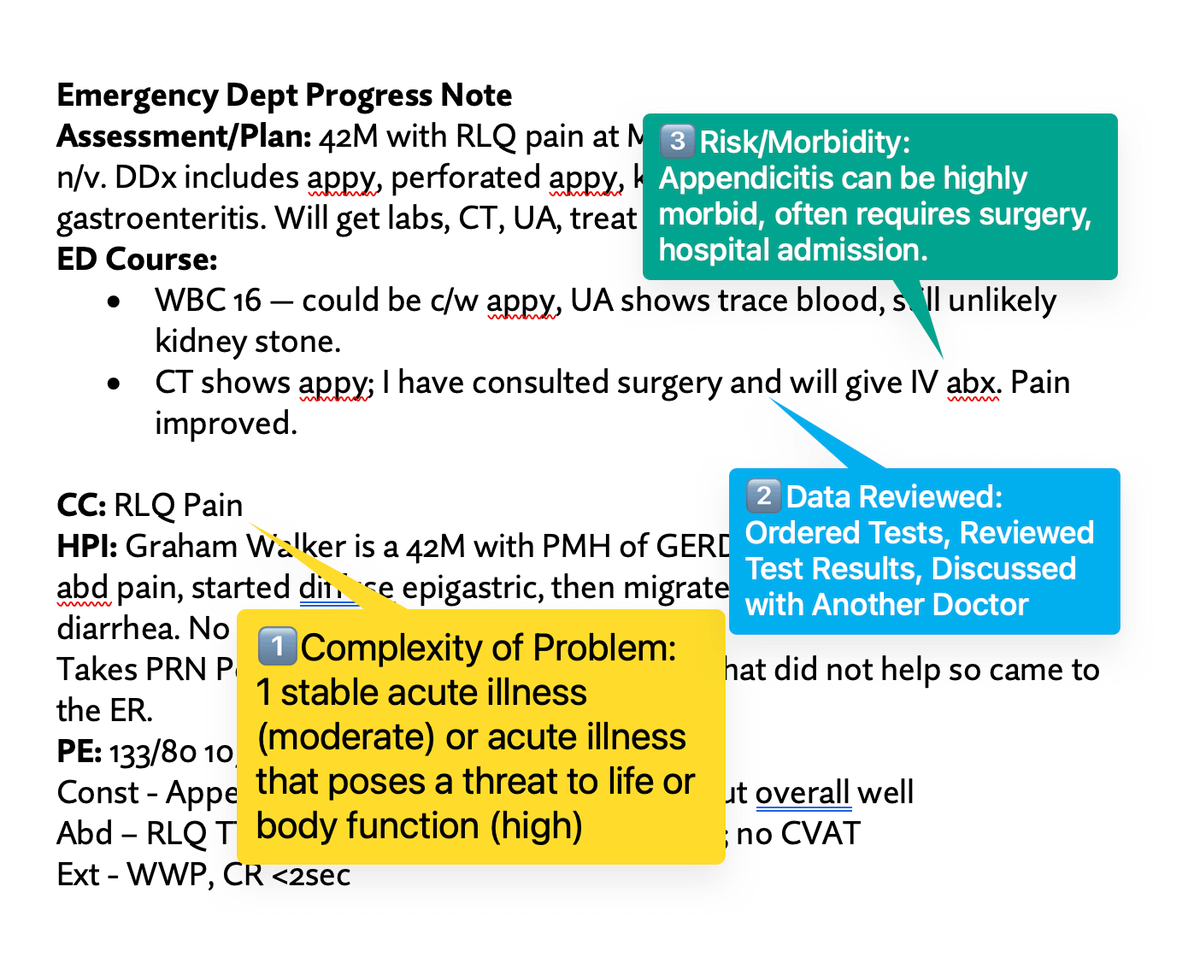
Now what I honestly don't know, as I'm not a documentation or coding expert, just a Very Basic ER Doctor:
➡️Do I have to document "Risk/Morbidity is high With Appendicitis" in order for it to count? I sure hope not, that seems repetitive and stupid.
➡️Same with adding some line about "I reviewed the patient's prior notes" in order for it to "count."
Still many questions. I'd love anyone who's actually an expert here to chime in here!
Let me try again, with another straightforward example: simple lac repair: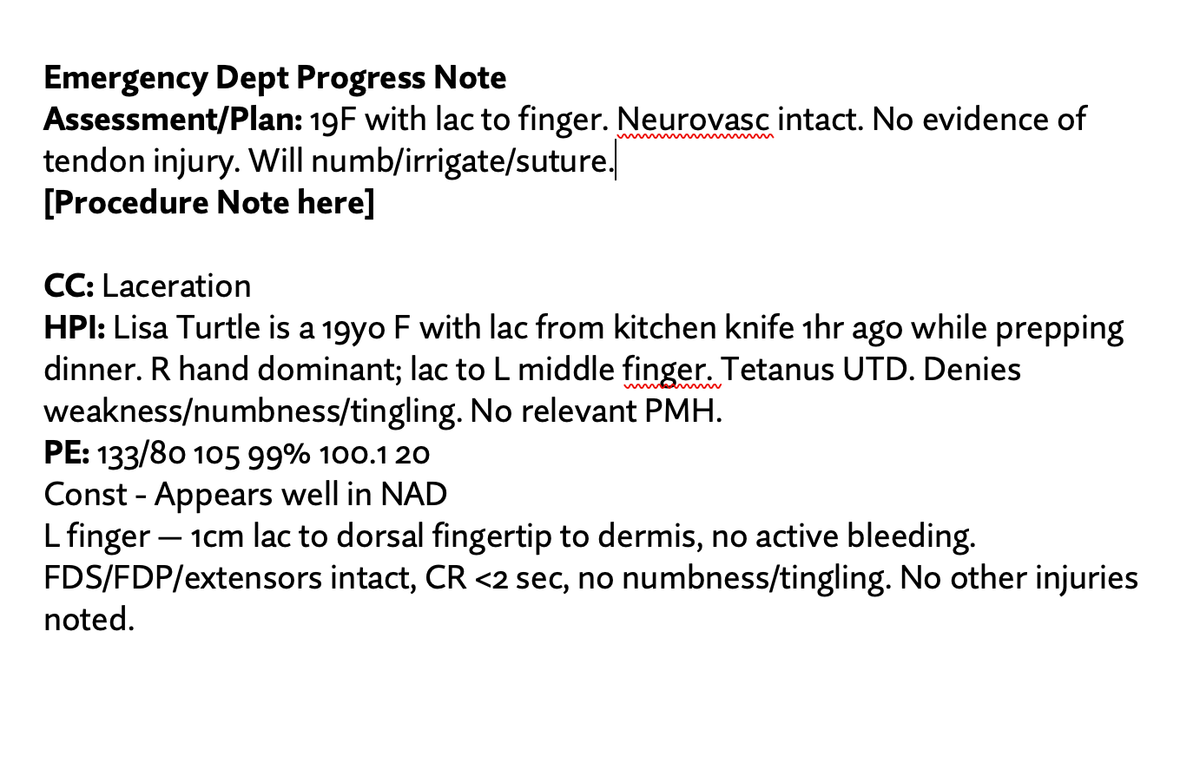
I think arguably this is either a Straightforward (99282) or a Low (99283) depending on interpretation and such, PLUS a simple lac repair procedure code.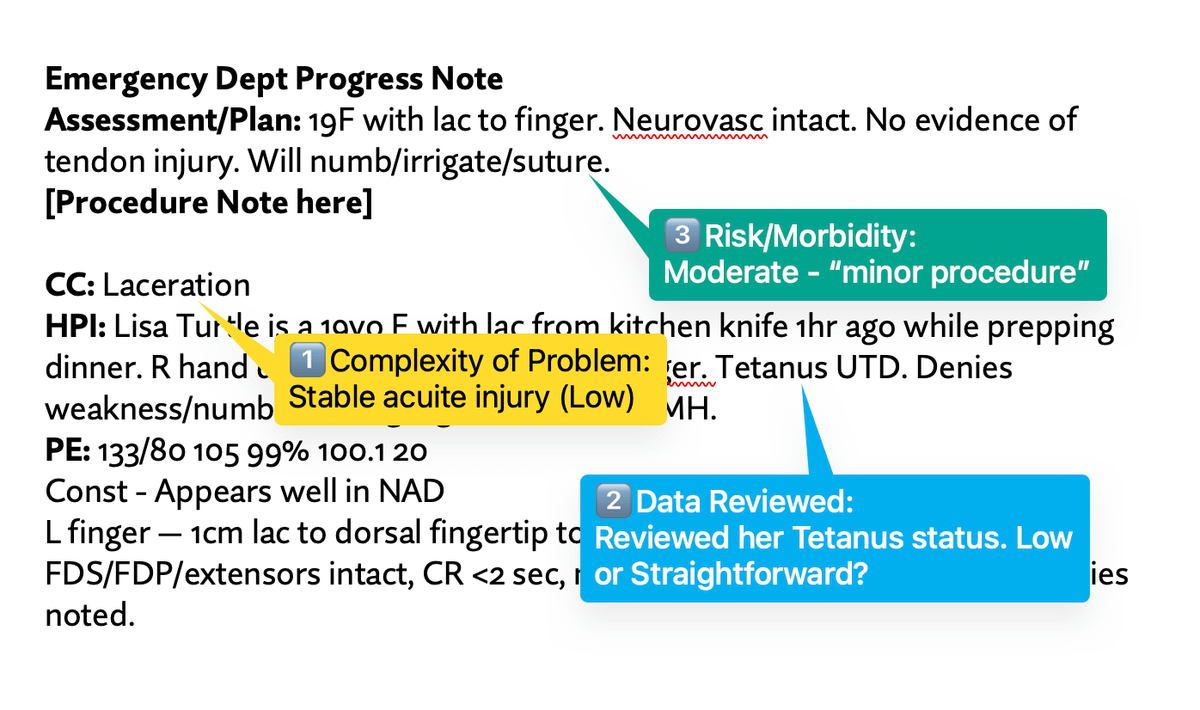
Overall I think this is going to be a major net WIN for emergency medicine. It will absolutely take some time for the specialty to get used to the MDM criteria, AND for us to de-clutter our notes, but even doing those two fake patient notes — it was much simpler/faster.
cc to people who commented
@ScholerinED @MDaware @Lgaard @gbosslet @mattjbrunner @reverendofdoubt and also @EdGainesIII who I feel like always knows about money stuff with emergency medicine

Graham Walker, MD
@grahamwalker
Emergency physician; I made @mdcalc; Tweets = my own/not employers'. Not a hero, just a well-trained human. So, so tired of COVID. #GetVaccinated 💉